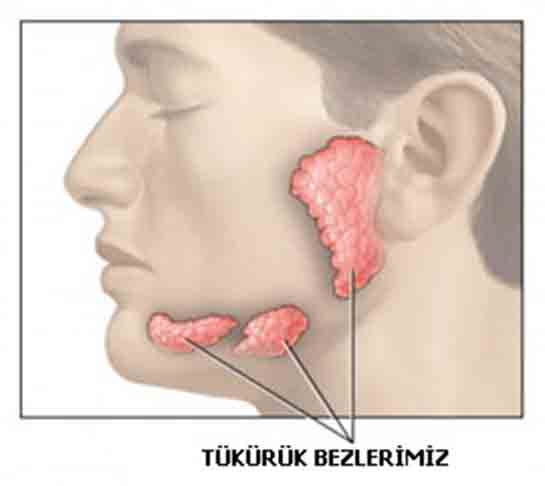
The salivary gland is a general name given to the tissues that secrete saliva. It is possible to divide the salivary glands into 4 groups under the name of salivary gland or diper. 3 of them pass as encapsulated tissues with different sizes and are called major salivary glands. If we look at the major salivary glands, these are the submandibular, parotid and sublingual glands. These major glands are two, right and left. The largest salivary glands are the Parotid. The parotids extend from the front of the auricle and cover the posterior part of the two cheeks in a splayed manner. However, they show an opening to the mouth part at the level of the second molar with a channel called the Stenon canal.
The facial nerve passes through the middle part of the parotid glands. The facial nerve and its parts, which are responsible for working the facial facial facial November muscles, divide the parotid gland into two parts, superficial and deep. The submandibular glands, aka the submandibular glands, are located on the right and left just below the jaw part. These glands are the size of a small plum. These glands open into the front part of the mouth thanks to a canal. We call this channel Wharton. The sublingual glands or sublingual salivary glands are located in the anterior lower part of the tongue and have two, right and left. The sublingual glands surround the maxillary gland duct at the base of the mouth. They look just like okra. They also show mouth opening with this channel. In addition to these major glands, there are many tiny salivary glands that are located scattered in the mucosa of the mouth and throat, especially in the cheek and palate. These glands are also called minor salivary glands. The secretion of the parotid is serous, that is, aqueous. The secretion of the sublingual and minor glands is in a coherent state, that is, mucous.
For diagnostic purposes, biochemistry laboratory tests are classically applied to the salivary glands, while imaging systems such as sialography, graphy, computed tomography, ultrasonography, magnetic resonance imaging are also included. In addition, fine needle aspiration with ultrasound accompaniment is also an important place in terms of diagnosis. But the diagnosis rate is lower than that of the thyroid. The probability of diagnosis of fine needle aspiration in salivary glands is generally high in tumoral diseases. However, this rate decreases in nontumoral diseases. There is no standard for applying an imaging system or fine needle aspiration before surgery. Each doctor applies his own method, taking into account the patient’s condition.
What are Salivary Gland Diseases?
It is necessary to evaluate salivary gland diseases in a wide way because there are many types. There may be many different disorders such as mumps, parotitis, sialolithiasis or sialadenosis with symptoms that may occur. But the most important thing to note here is the possibility that many different tumors, whether benign or bad, can develop in this area. It is possible to collect salivary gland diseases under two main headings under tumor and non-tumor diseases.
Non-Tumor Diseases
Mumps: If we are going to talk about non-tumor diseases, mumps or mumps virus can be considered cases of inflammation of the salivary glands. This condition is one of the childhood infectious diseases. Mumps often involves the parotid gland or glands, which causes swelling of the cheeks, while causing symptoms such as regional pain, malaise, fever. But along with these, there is also a quieter state of progression of the disease. It rarely holds other salivary glands, ovaries, testicles, tissues such as the central nervous system and pancreas.
The risks are conditions such as life risk that may occur due to meningoencephalitis, infertility due to orchitis and unilateral neurosensory hearing loss. Mumps plays an important role in unilateral neurosensory advanced or complete hearing loss that occurs during childhood. Treatment for mumps is diet, rest and pain medication. In case of orchitis, meningoencephalitis or hearing loss, hospitalization and extensive energetic treatments may be required.
Salivary Gland Stone: A salivary gland stone called sialolithiasis is a condition of stone development in the narrow channels that open the salivary gland or mouth. It often occurs in the submandibular glands and especially in their ducts. It can manifest itself in a rare way in the parotids, with an exceptional case in the sublingual and minor salivary glands. The reasons for the frequent formation of stones in the salivary glands under the jaw are that its secretion is thick, its duct is long, its content is rich in calcium-phosphate and hydroxyapetite. These substances form a nucleus. After a certain time, a stone called calculi begins to form around it.
Due to the high calcium content, submandibular stones are usually seen on an X-ray. On the contrary, parotid stones, on the other hand, are not usually seen on an X-ray because they contain low calcium. Submandibular gland stone, on the other hand, is seen in some periods with signs and symptoms such as swelling under the chin, increased complaints while eating, pain and decreased saliva passage through that channel. An under-jaw gland stone and a gland that grows or becomes inflamed with blockage may require surgical operation if there is no intervention against diet and massage practices. This is also done in the form of stone removal by endoscopic or classical method only with intervention in the canal. In addition, the gland can also be removed together with the canal.
Other Salivary Gland Diseases: Acute inflammation of the salivary gland with pus develops after a previous operation on the body or as a result of acute stasis in older people. In general, it holds the parotids. Treatment, on the other hand, can be considered as an application called energetic antibiotics, salivary gland massage, liquid supplementation, oral hygiene. Persistent inflammation of the salivary gland, that is, chronic sialadenitis, is observed due to acute inflammation that repeats itself, or a decrease in secretion accompanied by radiation therapy. In general, it holds the parotids. The treatment is for protection purposes. But if it is necessary, a superficial parotidectomy or low-dose radiation therapy may be performed.
Sialosis or sialadenosis, which we call salivary gland enlargement, is a bilateral growth without inflammation in the salivary glands due to diabetes, alcoholic cirrhosis, metabolic disorders or obesity. The treatment is aimed at the underlying cause. If necessary, total parotidectomy or superficial applications may be involved, at the risk of regrowth of the remaining gland tissues.
In branchial type I and branchial type II cysts, the condition occurs for lesions in the parotid region. It is the application of resections by preserving the facial nerve in its treatment. Salivary gland mucoceles are formed as a result of accumulation of mucous secretions with problems in ejaculation. In total, it can be seen in the entire oral mucosa, most often on the lips. Intraoral excision is performed as a treatment method. Marsupialization is required in the treatment of ranula, which is a salivary gland mucocele that develops as a bubble at the base of the mouth. In other words, it is the process of mouthing the cyst outwards. Recurrent parotid inflammation, called recurrent parotid, is a self-recurring inflammation in which the parotid glands, which often occur in children, are followed by attacks. It is tried to be stopped with deaths such as diet, massage, medication.
What is a Salivary Gland Tumor?
It is used to describe in general the tissues that develop in the major and minor salivary glands outside the control of the body. These tumors can be benign (selim) or malignant (malignant). These tumors are most often seen in the parotid gland. Although most of them are unlikely to turn into malignant, they are benign tumors called pleomorphic adenomas. If it is necessary to make a generalization, 80 out of every 10 salivary gland tumors are located in the parotid. 8 out of 10 parotid tumors are benign. Again, 8 out of 10 of the benign ones are pleomorphic adenomas.Tumors in the submandibular and submandibular glands are rarely observed. Despite this rare occurrence, almost half of the tumors are malignant. The majority of benign tumors under the jaw are composed of pleomorphic adenomas. But one of the points that should not be forgotten is the pathology of stones, although there is no tumor that is often seen in the submandibular gland. A serious part of minor ulcer gland tumors is malignant. However, these malignant tumors are rare.
When we look at its diversity, salivary gland tumors are incomparable with the situation in other tissues of the body. This condition can be explained as each tumor getting a source from one of the differentiated cells in the salivary gland, or each tumor getting a source from each other of two different stem cells found at different stages. We divided salivary gland tumors into benign and malignant. Benign tumors usually manifest themselves with the forties, while malignant tumors manifest themselves with the fifties.
Benign Tumors
If it is necessary to sort benign salivary gland tumors by their incidence, they are pleomorphic adenoma, warthin tumor and monomorphic adenomas. As the name suggests, pleomorphic adenoma or mixed tumor contains different cells in the salivary gland tissue, namely myopithelial, stromal and epithelial cells. Monomorphic adenomas, on the other hand, contain only one of the myopithelial or epithelial cell groups in a dominant way. However, there are also different types of benign tumors in the salivary glands, such as hemangiomas.